Rotator Cuff Impingement and Rotator Cuff Tears
Rob Parisien, MD, Maine Orthopaedic CenterShoulder pain is extremely common. It is estimated that up to 20% of the population will have an episode of significant shoulder pain in their lifetime. Shoulder pain accounts for approximately 5% of all visits to primary care physicians. To make matters worse, shoulder pain is often chronic. Up to 80% of patients with shoulder pain who see a physician have the pain for 6 months, and some patients have pain for years. While there are many different conditions that affect the shoulder, in this article, I want to focus on two of the more common and vexing problems: rotator cuff impingement and rotator cuff tears.
The rotator cuff is a group of 4 muscles and tendons that lie deep inside the shoulder. The tendons attach to the top of the humerus bone and help stabilize and move the upper arm. They are active with movements such as lifting your arm above your head, or reaching behind your back. The rotator cuff also acts as a cushion to help prevent the humerus from bumping into another bone deep inside the shoulder called the acromion. When the rotator cuff stops working properly, the two bones can bump into each other in an abnormal way, causing a condition known as “subacromial impingement syndrome”, which often contributes to rotator cuff damage, leading to a vicious cycle of damage and disability.
The rotator cuff can be damaged by an acute episode, such as a fall onto an outstretched shoulder. If the injury is severe enough, this can cause a complete tear with the development of significant pain and weakness. However, the most common way the rotator cuff becomes damaged is by chronic overuse. Repetitive overhead motion can lead to micro-tears of the rotator cuff, which can cause inflammation of the tendons and overlying lubricating layer called the subacromial bursa. If the aggravating condition continues, over time the tendons can weaken and tear either partially or fully. However, the rotator cuff and overlying bursa can cause pain even if it is not torn. Swelling and inflammation of the bursa can be very painful, and bone spurs and calcium deposits on the underside of the acromion (from chronic impingement) can contribute to the inflammatory process and cause pain.
The symptoms of rotator cuff impingement and rotator cuff tears can be varied, but usually pain with overhead activities is the hallmark. Pain at night is very common and usually indicates that the process is more advanced. Patients often have pain at night when lying in bed because the shoulder is not being pulled downward by gravity and the humeral head can bump into the acromion bone leading to a dull, aching type of pain. Some patients describe pain that is felt more in the arm, even going down almost to the elbow. Many patients also feel pain at the base of the neck. The rotator cuff is a deep structure, and, because of that, the pain may be hard to localize, making the symptoms all the more frustrating. When the rotator cuff is completely torn, patients will have weakness doing certain activities such as reaching out in front of the body or reaching overhead.
�
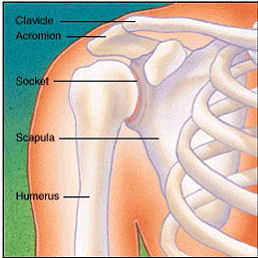 Normal Shoulder Joint |
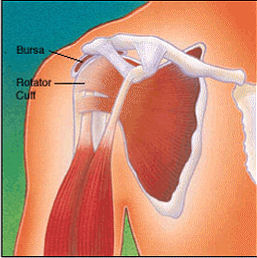 Normal Shoulder Muscles and Tendons |
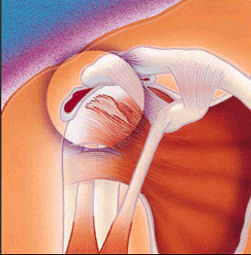 Impingement and Partial Rotator Cuff Tears |
A thorough physical exam by a skilled practitioner will usually be adequate to make the diagnosis of rotator cuff impingement syndrome and tears. Certain motions will be very painful in impingement syndrome, and characteristic weakness is found in patients with large tears. X-Rays are sometimes required to look for bone spurs and arthritis. Occasionally an MRI is used to identify tears in the rotator cuff tendons.
The treatment of impingement and rotator cuff tears is almost always conservative at first. Resting the shoulder and stopping aggravating activities is the first step. Physical therapy is often used to strengthen the rotator cuff muscles and other muscles around the shoulder. This can greatly diminish the symptoms by making the remaining rotator cuff more efficient and usually is all the intervention that is needed. Even patients with large rotator cuff tears can benefit from a few months of therapy from a good physical therapist. Occasionally however, this does not relieve the symptoms. In these cases, corticosteroid injections can help control the inflammation and relieve pain. Injections should be spaced apart by at least 2 to 3 months, and they can be quite effective. In general, no more than 3 injections should be given because too much medicine can weaken the remaining tendons.
If physical therapy and injections do not help, surgery is indicated. There are a number of surgical techniques used to treat these conditions, and the exact operation required depends upon the nature of the problem. In general, impingement syndrome is treated by decompressing the space above the humeral head. The bursa is removed and the bone spurs on the acromion are shaved to allow more space for the rotator cuff tendons. This can be done either arthroscopically (with 2 or 3 very small incisions) or open (with a single incision from 1-3 inches long). Many surgeons believe that the advantage of arthroscopic treatment is that there is less post-operative pain and can be done as day surgery. Complete rotator cuff tears are treated by suturing the torn tendon back to the humeral head. This can also be done either open or arthroscopically. There is considerable controversy in the orthopaedic literature about which way is best. The results are generally very good either way, with more than 85% of patients having considerable relief of their symptoms. Patients may be placed in a shoulder sling for a few days for a simple decompression or up to 6 weeks for a rotator cuff repair.
In summary, rotator cuff impingement syndrome and rotator cuff tears are very common problems and can be quite disabling. However, the conditions are treatable and many patients get complete relief with conservative, non-operative therapy. For the patient who does not get better with physical therapy or steroid injections, surgery can be very effective. For more information, an informative and trusted source is the American Academy of Orthopaedic Surgeons’ web site: http://orthoinfo.aaos.org.
Robert C. Parisien, MD, was raised in Auburn, Maine. He received his bachelor’s degree from the University of Colorado in Boulder and graduated with honors from Dartmouth Medical School in Hanover, New Hampshire. He did his internship in general surgery at Beth Israel Deaconess Hospital in Boston and completed his orthopaedic residency through the Harvard Combined Orthopaedic Residency Program, serving as chief orthopaedic resident at Massachusetts General Hospital from January to June of 2004. He completed a Sports Medicine Fellowship at Harvard in December of 2004.
Used with permission from the American Academy of Orthopaedic Surgeons, https://orthoinfo.aaos.org/ web site.
Herb's Tips and More
-
 Did you know that you can make soap, candles and lotion with your herbs?
Did you know that you can make soap, candles and lotion with your herbs? -
 Never take any herb identity for granted. The best way to be sure that you are using the right kind of herb is by buying it.
Never take any herb identity for granted. The best way to be sure that you are using the right kind of herb is by buying it. -
Excellent health articles whether you are looking for information or inspiration regarding preventive health or are dealing with a medical
challenge.









